
Parkinson’s disease is a degenerative disorder of the central nervous system long-term and directly affects the motor system. Symptoms generally appear slowly over time. Early in the disease, the most obvious are tremors, stiffness, slow movement, and difficulty walking, thinking, and behavioral problems can also occur. Dementia becomes expected in the advanced stages of the disease, and depression and anxiety are also common in more than one-third of people.
It is the second most common neurodegenerative disorder. The progress of Parkinson’s disease and the degree of deterioration and damage vary from individual to individual. That is, not everyone happens in the same way. Many people with this disease live long, productive lives, while others become incapacitated much more quickly; premature death is usually due to complications related to falls or pneumonia.
Most of the people who develop Parkinson’s are 60 years or older. Since the general life expectancy is increasing, the number of people with this disease will increase in the future. Adult-onset is the most common, but early-onset Parkinson’s disease (between 21-40 years) and juvenile-onset (before 21 years).
Index
History of Parkinson’s disease
In 1817, an English physician, James Parkinson, published his essay reporting six cases of agitant paralysis. An Essay on Shivering Paralysis described the characteristic resting tremor, abnormal posture and gait, paralysis, decreased muscle strength, and how the disease progresses over time. The earliest neurologists to make further additions to knowledge of the disease include Trousseau, Gowers, Kinnier Wilson, and Erb, and most notably Jean-Martin Charcot, whose studies between 1868 and 1881 were a milestone in understanding the disease.
Among other advances, he distinguished between stiffness, weakness, and bradykinesia and defended the change of name of the disease in honor of James Parkinson.
In 1912, Frederic Lewy described microscopic particles in affected brains, later called “Lewy bodies.” In 1919 Konstantin Tretiakoff reported that the substantia nigra was the main affected brain structure. Still, this finding was not widely accepted until it was confirmed by other studies published by Rolf Hassler in 1938. The underlying biochemical changes in the brain were identified in the decade 1950, primarily due to the work of Arvid Carlsson on the neurotransmitter dopamine and Oleh Hornykiewicz on its role in Parkinson’s disease. In 1997, alpha-synuclein was the main component of Lewy bodies by Spillantini, Trojanowski, Goedert, and others.
Anticholinergics and surgery (injury to the corticospinal tract or some of the basal ganglia structures) were the only treatments until the arrival of levodopa, which dramatically reduced its use. Levodopa was first synthesized in 1911 by Casimir Funk, but received little attention until the mid-20th century, entered clinical practice in 1967, and sparked a revolution in the treatment of Parkinson’s. In the late 1980s, deep brain stimulation introduced by Alim Louis Benabid and his colleagues in Grenoble, France, emerged as a possible treatment.
Causes of Parkinson’s disease
Environmental factors
Exposure to pesticides and a history of head injury have been linked to the disease, but the risks are modest. Smoking cigarettes and caffeinated drinking beverages are also associated with small increases in the risk of developing it.
Low urate concentrations in the blood serum are associated with an increased risk.
Genetics
Research indicates that it is the product of a complex interplay of genetic and environmental factors. About 15% of people with Parkinson’s disease have a first-degree relative with the disease, and 5-10% of people with Parkinson’s are known to have forms that occur due to a mutation in one of several genes specific. Harboring one of these genetic mutations may not lead to disease; susceptibility factors put the individual at increased risk, often in combination with other risk factors, affecting the age of onset, severity, and progression.
Several genes related to Parkinson’s are involved in the function of lysosomes, organelles that digest cell waste products. It has been suggested that some cases may be caused by dysfunctions of the lysosomes that reduce the ability of cells to break down alpha-synuclein.
Parkinson’s disease is idiopathic in most individuals, meaning it occurs sporadically with no known cause. However, some people diagnosed with Parkinson’s also have relatives with the disease. Scientists have identified several genes associated with the disorder by studying families with inherited conditions. Studying these genes helps to understand the cause of the disease and can lead to new therapies. So far, five genes have been identified associated with Parkinson’s disease.
- SNCA (synuclein, non-A4 alpha component of the amyloid precursor): Produces the alpha-synuclein protein in human brain cells, this protein aggregates in groups called Lewy bodies. Mutations are found in early-onset diseases.
- PARK2 ( Juvenile autosomal recessive Parkinson’s disease 2): PARK2 gene mutations are found primarily in individuals with juvenile Parkinson’s disease.
- PARK7 (Autosomal recessive Parkinson’s disease, early-onset 7): PARK7 mutations found in early-onset Parkinson’s disease produce the DJ-1 protein, which can protect cells from oxidative stress.
- PINK1 (putative PTEN-induced kinase 1): Mutations in this gene are found early on. The exact function of the protein made by PINK1 is not known, but it may protect structures within the cell called mitochondria from stress.
- LRRK2 (Leucine-rich repeat kinase 2): Mutations in the LRRK2 gene have been linked to late-onset Parkinson’s disease.
Symptoms of Parkinson’s disease
The main symptoms of the disease are related to voluntary and involuntary motor function and usually start on one side of the body. Symptoms are mild at first and will progress over time; some people are more affected than others.
Studies have shown that by the time the primary symptoms appear, people will have lost 60% to 80% or more of the dopamine-producing cells in the brain. Characteristic motor symptoms include the following:
Temblor
They often appear in a hand, arm, or leg, occur when you are awake, sitting, or standing (rest tremor), and improve when you move that part of your body.
Tremor is often the first symptom that people with Parkinson’s disease or their family members notice. It can affect the chin, lips, and tongue. Tremors can be worse when an individual is excited, tired, or stressed.
Rigidity
Stiffness of the limbs and trunk, which may increase during movement, can cause muscle aches and pain. Loss of fine hand movements can lead to cursive writing (micrograph) and make feeding difficult.
Bradykinesia
It is the slowness with which a voluntary movement occurs. Over time, it can be challenging to initiate and complete it. Bradykinesia, along with stiffness, can also affect the facial muscles and result in a blank, “mask-like” appearance.
Postural instability
Damaged or lost reflexes can make it difficult to adjust posture for balance. Postural instability can lead to falls.
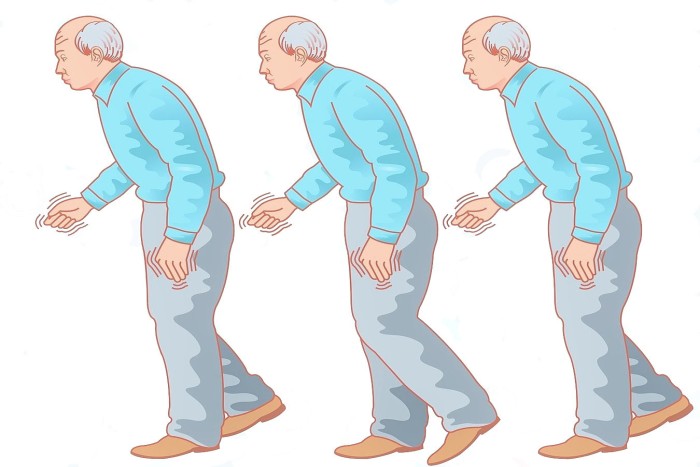
Parkinsonian onset
People with more progressive Parkinson’s disease develop a distinctive gait from walking with a stooped position and a decreased or absent arm swing. It can be difficult to start walking and turning around. People can freeze midway and appear to fall when walking.
Others
In addition to the above symptoms, it can affect other functions.
The problems with sleep are characteristic of the disease and can worsen with medication. Symptoms can manifest as daytime sleepiness (including sudden sleep attacks that resemble narcolepsy ), disturbances in sleep, or insomnia. Behavioral disorder, in which patients act out dreams, sometimes injuring themselves or their bed partner, can begin many years before developing motor or cognitive characteristics.
Alterations in the autonomic nervous system can cause orthostatic hypotension (low blood pressure when standing), oily skin and excessive sweating, urinary incontinence, and impaired sexual function. Constipation and disturbed stomach emptying (gastric dysmotility) can be severe enough to cause discomfort and even endanger health. Changes in perception can include an impaired sense of smell, impaired vision, pain, and paresthesia (tingling and numbness). All of these symptoms can occur years before the diagnosis of the disease.
What other conditions are similar to Parkinson’s disease?
It can be similar to several conditions with very similar symptoms known as Parkinsonism in its early stages. These conditions include multisystemic atrophy, progressive supranuclear palsy, corticobasal degeneration, dementia with Lewy bodies, stroke, encephalitis (brain inflammation), and head trauma.
Alzheimer’s and primary lateral sclerosis have also been confused with Parkinson’s disease. Other similar conditions include essential tremor, dystonic tremor, vascular Parkinsonism, and drug-induced Parkinsonism.
Diagnosis of Parkinson’s disease
A physician will initially evaluate with a careful medical history and neurological examination. People can be given levodopa, with any resulting improvement in motor impairment that helps confirm the diagnosis of Parkinson’s disease. The finding of Lewy bodies in the midbrain at autopsy is generally considered the final proof that the person has this disease.
The clinical course of the disease over time may reveal that it is not, requiring that the clinical presentation be reviewed periodically to confirm the accuracy of the diagnosis.
Other causes that can secondarily cause parkinsonism are strokes and drugs. Parkinson plus syndromes, such as progressive supranuclear palsy and multisystemic atrophy, should be ruled out.
When diagnoses are controlled by autopsy, movement disorder experts are 79.6% accurate in the initial assessment and 83.9% accurate after refining their diagnosis in a follow-up examination. When clinical diagnoses performed mainly by inexperienced people are controlled by autopsy, the average precision is 73.8%. Overall, 80.6% of diagnoses are accurate.
Computed tomography
It has become more accurate in diagnosing the disease over time, specifically through iron-sensitive sequences with a magnetic field intensity of at least 3T. It is also used to rule out other conditions that may be secondary causes of parkinsonism, more frequent encephalitis, chronic ischemic insults, and less frequent entities such as basal ganglia and hydrocephalus tumors.
Who is at risk for Parkinson’s disease?
Age is the most significant risk factor for the development and progression of the disease. Most of the people who develop it are over 60 years of age.
Men are affected about 1.5 to 2 times more often than women.
A small number of people are at increased risk due to a family history of the disorder.
Head trauma, illness, or exposure to environmental toxins such as pesticides and herbicides can be a risk factors.
Prevention of Parkinson’s disease
Exercise in later life can reduce the risk of Parkinson’s disease later in life. Caffeine also appears to be more protective, with a more significant decrease in risk occurring with a higher intake of caffeinated beverages, such as coffee. People who smoke cigarettes or use smokeless tobacco are less likely than non-smokers to develop Parkinson’s disease. The more they have used tobacco, the less likely they will develop Parkinson’s disease. It is not known what underlies this effect.
Antioxidants, such as vitamins C and E, have been proposed to protect against disease, but study results have been conflicting, and no positive effect has been shown.
The results regarding fat and fatty acids have been conflicting, with several studies reporting protective effects, risk-increasing effects, or no effect. There have been preliminary indications that anti-inflammatory drugs and calcium channel blockers may be protective. A 2010 meta-analysis found that non-steroidal anti-inflammatory drugs (other than aspirin) have been associated with at least a 15 percent reduction in the incidence of the development of Parkinson’s disease.
Treatment for Parkinson’s disease
Today there is no treatment to cure the disease. Several therapies are available to delay the onset of motor symptoms and improve them somewhat. These therapies are designed to increase the amount of dopamine in the brain, either by replacing dopamine, mimicking it, or prolonging the effect by inhibiting its breakdown. Studies have shown that early therapy in the non-motor stage can somehow delay the onset of motor symptoms, thus extending people’s quality of life.
Treatments for Parkinson’s include:
- Medications: such as levodopa and dopamine agonists. This is the most common and used treatment for this disease.
- Home treatment: You can take many steps at home to make it easier to treat your symptoms, such as exercising regularly and following a healthy diet.
- Surgery: Brain surgery, for example, deep brain stimulation, may be considered when medicine fails to control symptoms or causes severe or disabling side effects.
- Speech therapy: Speech therapists use breathing exercises to help you overcome the soft, imprecise speech and monotonous voice that develops in advanced Parkinson’s disease.
- Physical therapy: Therapists can help you improve how you walk and reduce the risk of falls.
- Occupational therapy: Therapists can help you learn new ways of doing things for yourself to stay independent longer.
- Treatment for mental problems: You or your family members may notice that you begin to have problems with memory, problem-solving, learning, and other cognitive functions. When these problems prevent you from doing daily activities, it is dementia. Some medicines can help treat dementia in people with Parkinson’s.

Hello, how are you? My name is Georgia Tarrant, and I am a clinical psychologist. In everyday life, professional obligations seem to predominate over our personal life. It's as if work takes up more and more of the time we'd love to devote to our love life, our family, or even a moment of leisure.